The Japanese nursing care insurance functions well. It changed a system of health care for elderly. In compare with it, The Japanese welfare system for children who require medical devices and care is delayed
The Japanese welfare system is not made to assume these children.
One critical problem is that there is no system to connect medical and welfare. There is no function equivalent to what care managers are in Japanese nursing care insurance. As home-visit nursing is covered by medical insurance system, it is difficult to coordinate with welfare system. Infants are out of the system from the beginning, so we cannot utilize helpers. We have insufficient day-care or short stay facilities. Commuting may be difficult. These are the common problems. The complex relationship between the doctors in community, hospitals and development facilities makes the problem that it is unclear which doctor is primary. Due to the personal information protection policy limiting ways to share information to phone calls and documents makes communication difficult between them.
Here, you can see the summary of current status of regional medical/livelihood support in Japan.
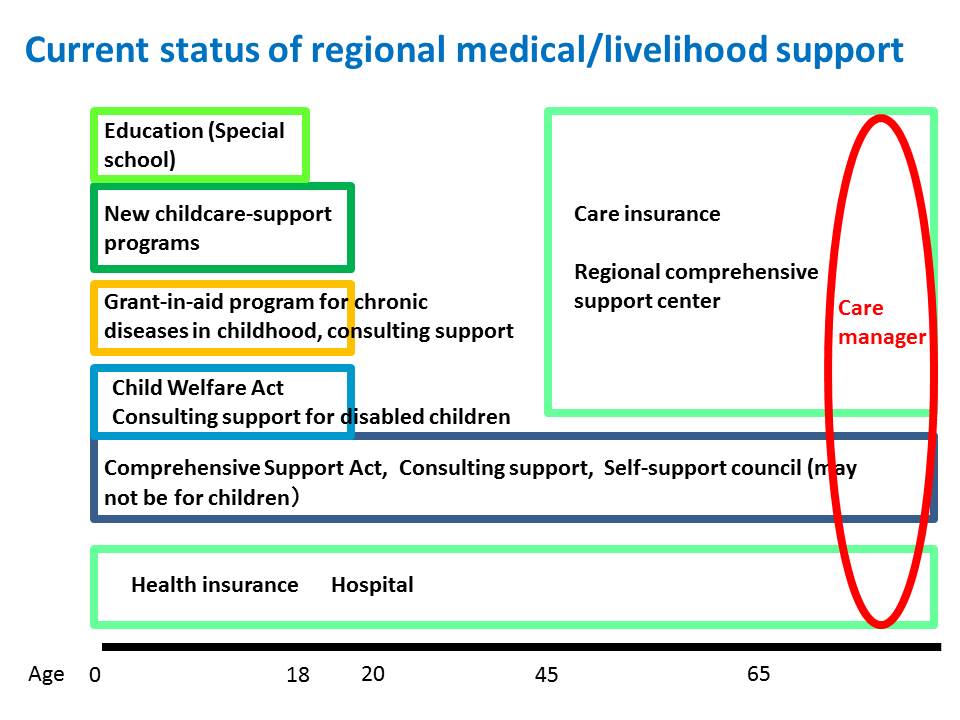
For adults, the system is well organized with medical insurance, nursing care insurance and the bridge between the two. On the other hand, for children, we have several systems in place but there is no coordinating mechanism between them, which makes the entire system hard to understand and confusing.
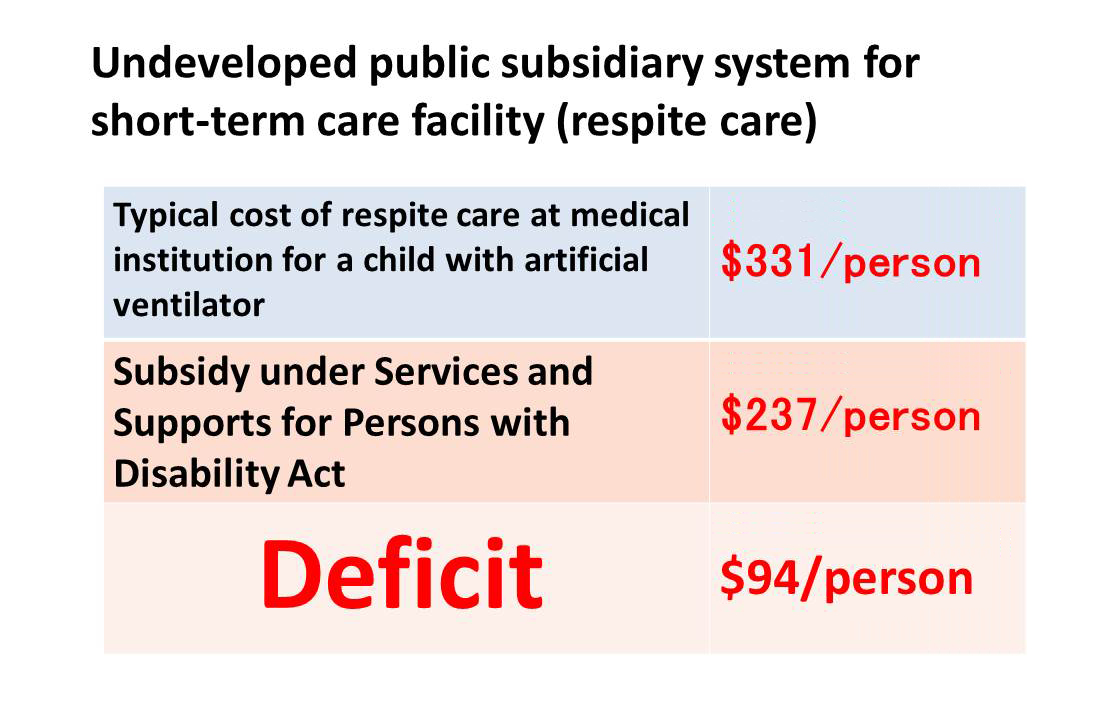
There is insufficient public financing system for respite care. In particular, on the welfare service for the disabled, the subsidy for respite care barely covers the cost for a child without ventilation. As you can see on this table, if you have a child with ventilation respite care costs deficit about 100 dollars a day, the government does not provide that.
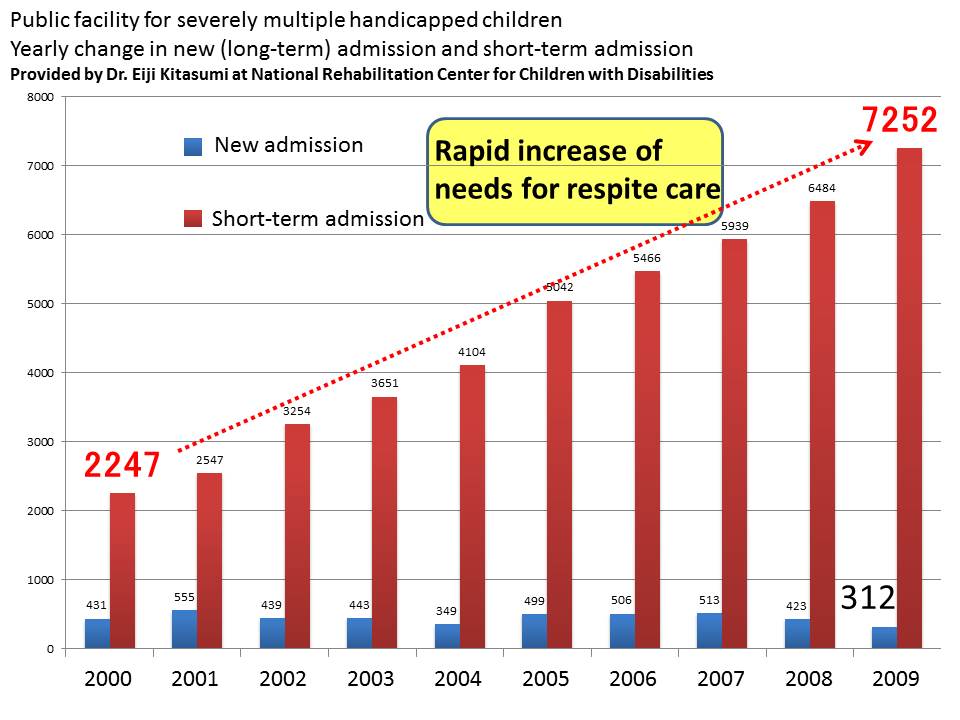
On the other hand, the need for respite care is rapidly increasing. This data is from Dr. Kitazumi,director at National Rehabilitation Center for Children with Disabilities. You can clearly see the rapid increase of the need for respite care in the last decade.
As shown here, in Tokyo there is a severe shortage of respite care facilities. It is far from satisfying its need.

In the framework of child home care, how should regional comprehensive care be achieved? How should we coordinate different professions?
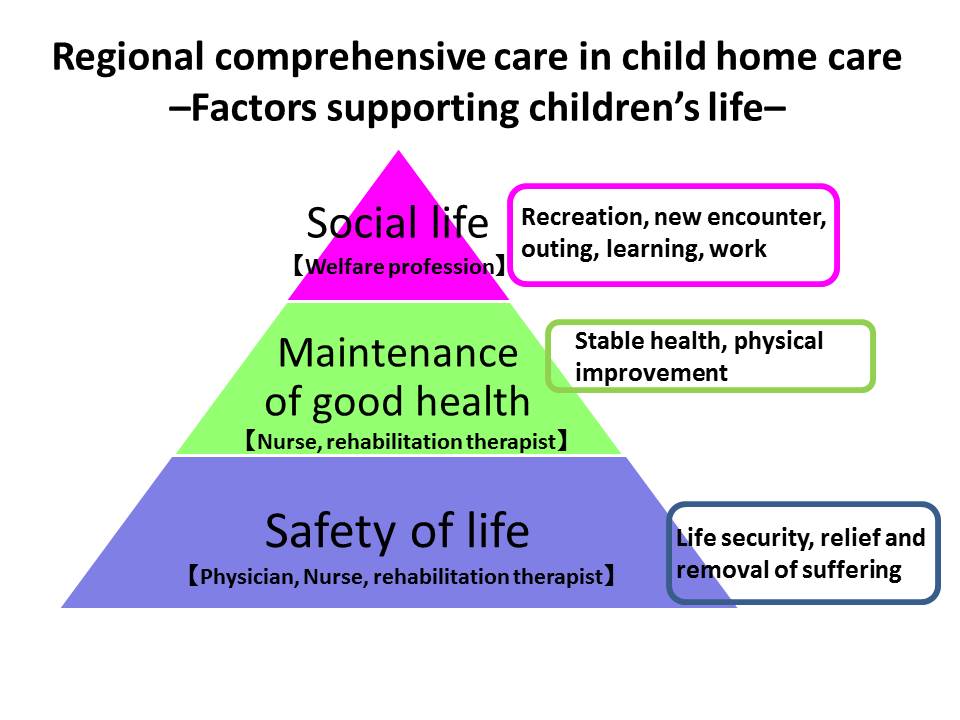
At the level of individual children, protecting their lives comes first. We need to ensure stable and safe operation of medical devices such as artificial ventilator in both local community and home, as well as proper control of spasm and infection. These are primarily physician’s job. In addition, we need to promote the children’s health. For example, we want to make sure that their bodies stay healthy and not get cold when they go outside. Nurses and rehabilitation therapists play a major role for this. Finally, we want the children have valued roles to experience and lean new things, meet new people, and have fun. This is achieved through livelihood support and welfare.
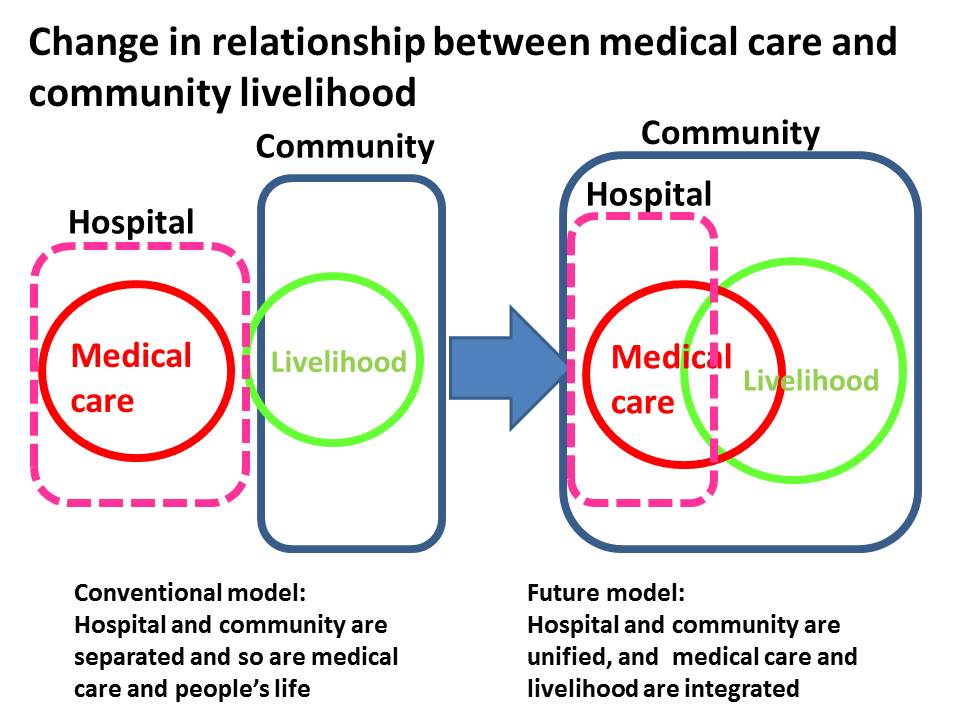
In Japan, medical care has separated itself from and people’s livelihood in the past several decades. But now, a big change is about to happen thanks to a national-level effort to promote in-home medical care. We are now transitioning from a world of ‘medical-livelihood separation’ to ‘medical-livelihood integration’. This shift means that hospitals and communities become connected together, leading to a next-generation medical model where medical care and community’s livelihood are tightly integrated. This is in fact a big challenge not only for child medical care but also for adult medical care.